Sheena Byrom Joins Our Advisory Panel
We are delighted to announce the appointment of consultant midwife and lifelong campaigner for positive childbirth, Sheena Byrom OBE to our Advisory Panel. Sheena Byrom… Read More


We are delighted to announce the appointment of consultant midwife and lifelong campaigner for positive childbirth, Sheena Byrom OBE to our Advisory Panel. Sheena Byrom… Read More
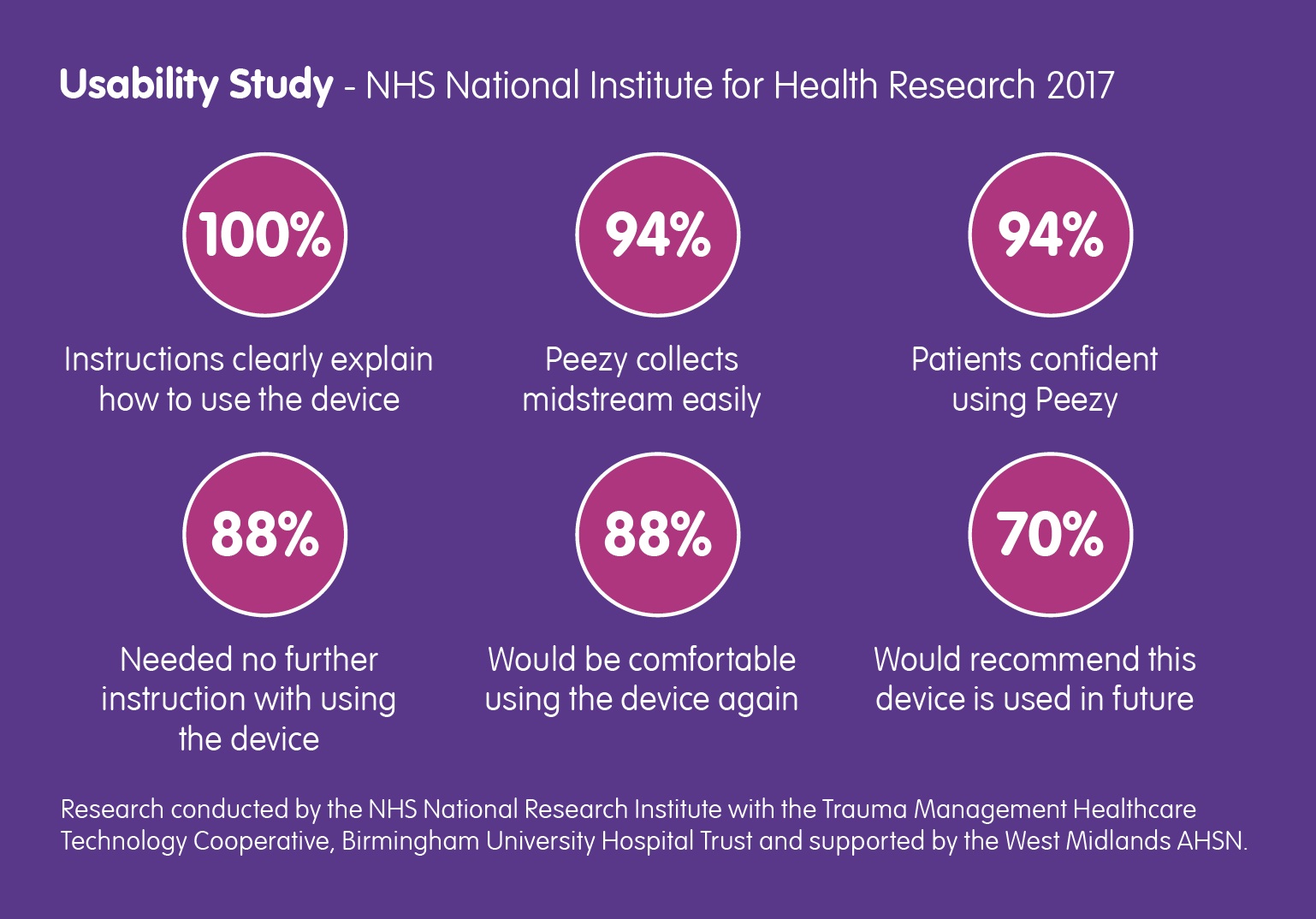
Back in March of this year, the NHS National Institute for Health Research contacted Forte Medical, asking for a case study… Read More
We’ve been an advocate for the MUST Campaign since they launched in May and this article explains why it is so important. Read about it… Read More

This week saw the launch of Forte Medical’s Series A investment round for growth, export and new product development. Seeking £3.5m, the company is engaging… Read More

Barry Shrier, Founder of annual health innovation event Giant Live, presents the third Disruptor Giant Health Innovators TV interview featuring Giovanna Forte, CEO of Forte… Read More

How easy is Peezy? Very! Click here to see our new animation showing five simple steps that deliver right-first-time urine specimen collection. Any clinician… Read More
Antibiotic resistance in children’s E. coli, a bacteria that is the most common cause of urinary tract infection, is high against many antibiotics commonly prescribed in… Read More

Doctors can tell a lot about your health from your urine sample, if taken properly. Insightful piece by Rob Eley and Michael Sinnott from The… Read More

It costs so little to put it right: “The NHS spent £434 million in 2013/14 on treating184,000 patients in unplanned admissions associated with a UTI. … Read More

Encouraged by the growing national recognition of the value of urine in diagnostic medicine, health leaders are being approached to join a new Forte Medical… Read More
