IPC 2019 – We’re Exhibiting!
The future of preventative care, infection control, antimicrobial resistance and patient safety are routinely undermined by lazy attitudes towards urine collection, the most common diagnostic… Read More

The future of preventative care, infection control, antimicrobial resistance and patient safety are routinely undermined by lazy attitudes towards urine collection, the most common diagnostic… Read More
We are delighted to announce the appointment of consultant midwife and lifelong campaigner for positive childbirth, Sheena Byrom OBE to our Advisory Panel. Sheena Byrom… Read More

The latest issue of Urology News features an interesting and important conversation with Urological Consultant Mr Ased Ali about the importance of urine in diagnosis… Read More

Amongst British adults, urology diseases such as testicular cancer and prostate cancer are not well understood and men are not looking out for the signs… Read More

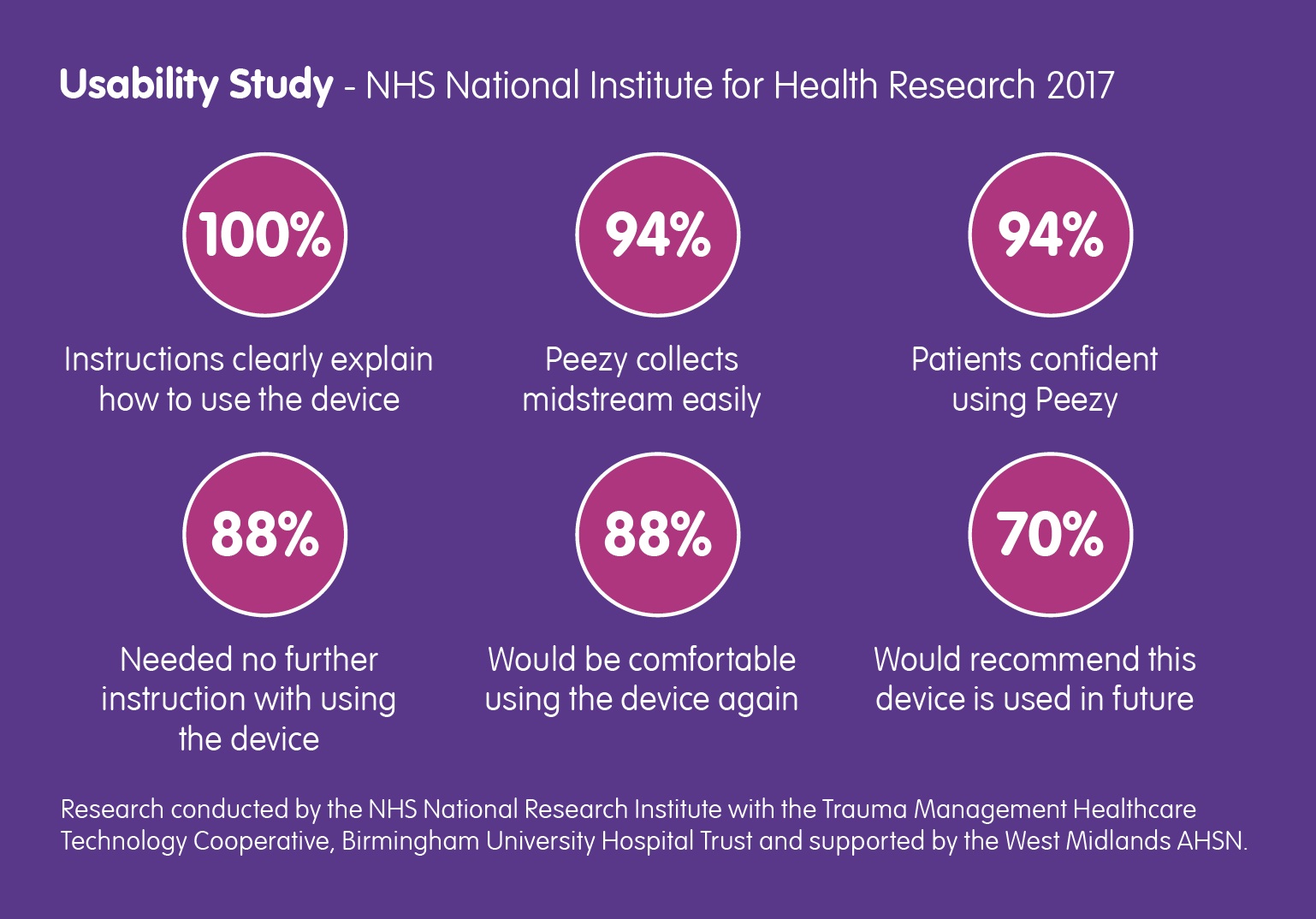
Back in March of this year, the NHS National Institute for Health Research contacted Forte Medical, asking for a case study… Read More
We’ve been an advocate for the MUST Campaign since they launched in May and this article explains why it is so important. Read about it… Read More

The inaugural speech delivered by Mr Matt Hancock upon his appointment as Secretary of State for Health, focused quite rightly on the… Read More
Barry Shrier, Founder of annual health innovation event Giant Live, presents the third Disruptor Giant Health Innovators TV interview featuring Giovanna Forte, CEO of Forte… Read More

In elderly patients, a UTI can induce behaviour that may be interpreted as “challenging”. As millions of us know, UTI is at best uncomfortable, at… Read More
Symptoms of urinary tract infections can be acute and in many cases, very debilitating. The need for a protocol around the collection of urine specimens… Read More