Urine Is Liquid Gold When It Comes To Testing
Today’s Hippocratic Post features an overview on the importance of urine and the evidence supporting why our technology plays such a vital role in… Read More


Today’s Hippocratic Post features an overview on the importance of urine and the evidence supporting why our technology plays such a vital role in… Read More
We attended the ABHI Parliamentary Reception last night and CEO Giovanna Forte had the opportunity to speak with The Rt Hon Matt Hancock MP, Secretary… Read More
The future of preventative care, infection control, antimicrobial resistance and patient safety are routinely undermined by lazy attitudes towards urine collection, the most common diagnostic… Read More
Giovanna Forte, CEO was delighted to be one of 10 British executives to make their way to UC Irvine (UCI) for the Greater Irvine Chamber’s… Read More

The latest issue of Urology News features an interesting and important conversation with Urological Consultant Mr Ased Ali about the importance of urine in diagnosis… Read More

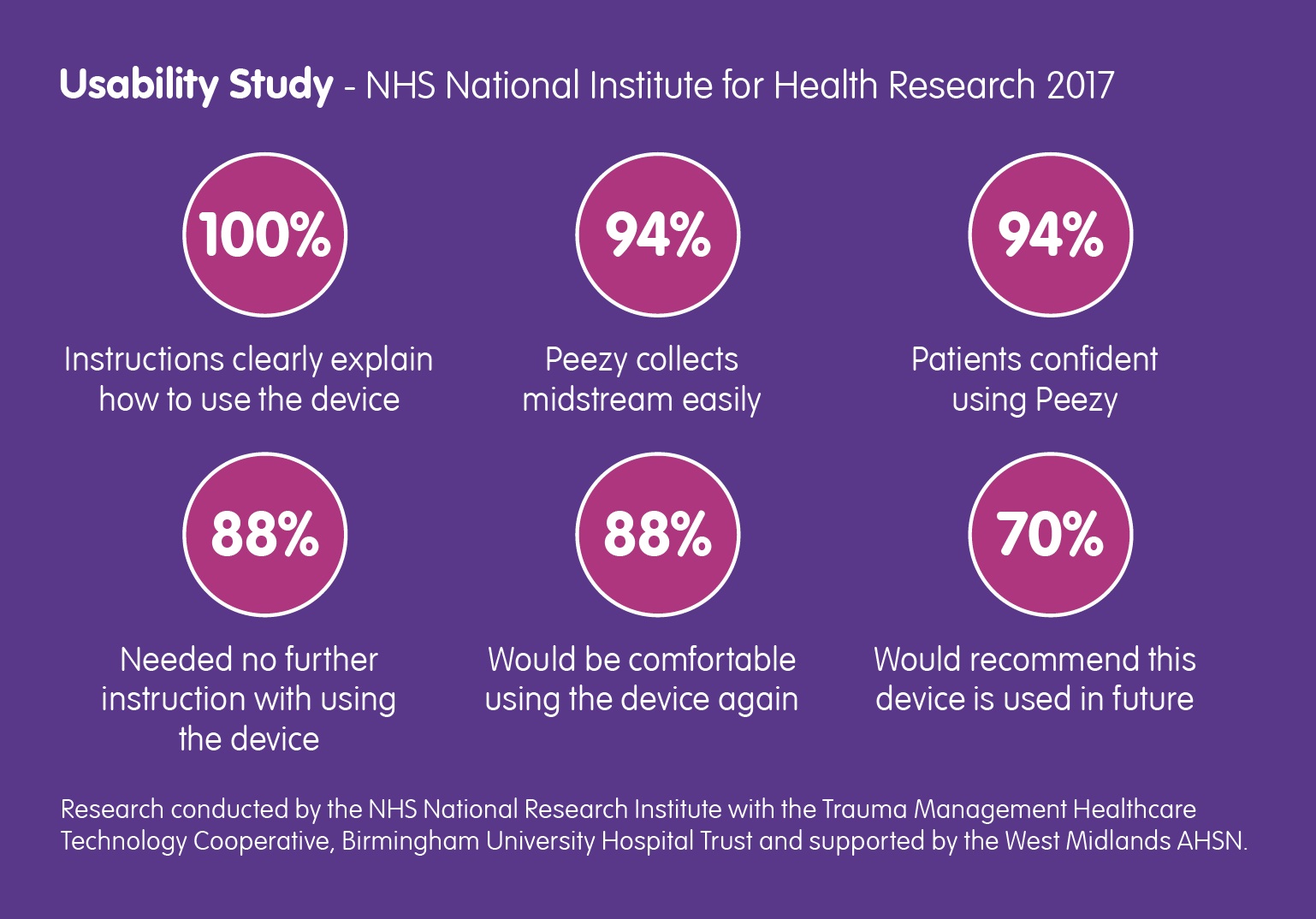
Back in March of this year, the NHS National Institute for Health Research contacted Forte Medical, asking for a case study… Read More
This is the latest recommendation following publication of a Californian study about the rise of antibiotic-resistant bacteria. But right-first-time diagnosis and treatment is only… Read More

A new study shows that Antibiotic-resistant UTI bacteria is becoming more common; Knowlex has created a short-film about the research and what you should know… Read More
The inaugural speech delivered by Mr Matt Hancock upon his appointment as Secretary of State for Health, focused quite rightly on the… Read More
Barry Shrier, Founder of annual health innovation event Giant Live, presents the third Disruptor Giant Health Innovators TV interview featuring Giovanna Forte, CEO of Forte… Read More
